prostate cancer
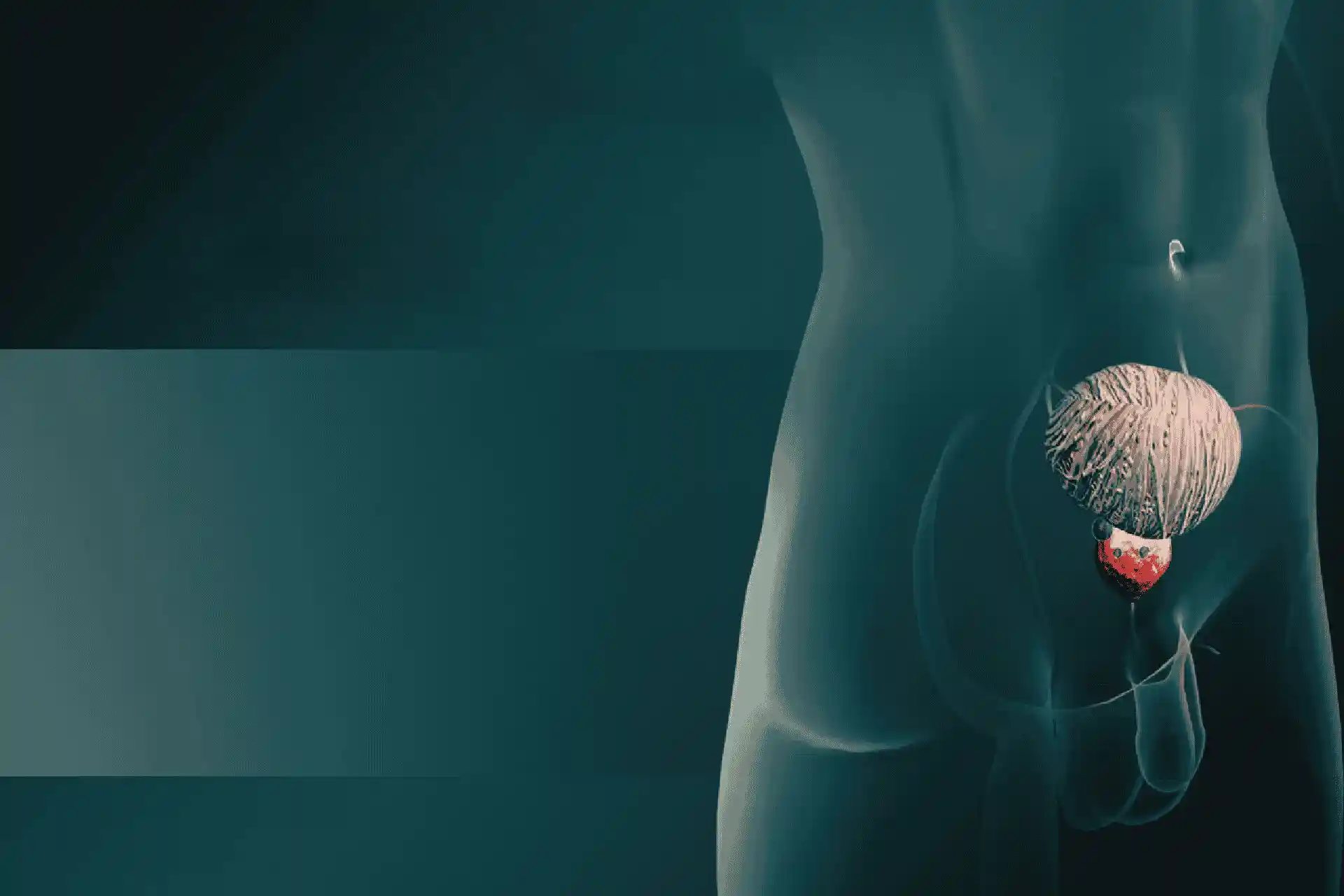
Prostate cancer is the abnormal growth of cells in the prostate gland. The prostate gland is a small walnut-shaped gland located behind the testicles in men. It produces the seminal fluid that
nourishes and transports sperm.
Prostate cancer is one of the most common cancers in men. The exact cause of prostate cancer is unknown, but it may be linked to age, family history, and certain genetic factors.
Typically, prostate cancer grows very slowly and may not cause any symptoms for many years. As the cancer progresses, it can cause symptoms such as:
- Need to urinate frequently, especially at night
- Difficulty starting urination or holding back urine
- Weak or interrupted urine stream
- Painful or burning urination
- Difficulty having an erection
- Painful ejaculation
- Blood in the urine or semen
- Frequent pain or stiffness in the lower back, hips, or upper thighs
Prostate cancer diagnosis is based on a digital rectal exam, blood test for prostate specific antigen (PSA), and a biopsy of prostate tissue. Imaging tests such as MRI, CT scan, and bone scan may
also be used to determine the stage and spread of the cancer.
Treatment options for prostate cancer include:
- Active surveillance: Closely monitoring the cancer and providing treatment only if it progresses. This is often done for older men with early stage cancer.
- Radiation therapy: Using high-powered energy beams to kill cancer cells. This can be done by external beam radiation or brachytherapy (implanting radioactive seeds in the prostate).
- Surgery: Removing the prostate gland (radical prostatectomy) using open or laparoscopic techniques. It can be done to remove the complete prostate or only part of it.
- Hormone therapy: Reducing testosterone levels to shrink or slow the growth of prostate cancer. This can be done using medications or surgery (orchiectomy to remove testicles).
- Chemotherapy: Using anti-cancer drugs to destroy cancer cells. Chemotherapy is usually given when the cancer has spread outside the prostate gland.
- Cryotherapy: Freezing and destroying cancer cells using extremely cold temperatures. It is less invasive than surgery but has more side effects.
- High intensity focused ultrasound (HIFU): Using high energy ultrasound waves to heat and destroy cancer cells. It is non-invasive but still experimental.
- Vaccine treatment: Stimulating the body's own immune system to attack prostate cancer cells. Prostate cancer vaccines are still being researched.
Regular follow-up tests are required after treatment to check for cancer recurrence. With treatment, prostate cancer can typically be managed effectively.
Transcript:-
The prostate gland is a part of the male reproductive system. It functions in the production and storage of semial fluid and as an exocrine gland.
Located within the pelvis, this gland measures three centimeters long, encircling the urethra distal to the urinary bladder, and anterior to the rectum. Prostate cancer, most often referred to as
adenocarcinoma or glandular carcinoma, arises in the peripheral zone from se secreting prostate gland cells that become cancerous. The cancerous cells are initially local. But then multiply and invade
into the St. Stroma forming a tumor.
The prostate tumor commonly invades the rectum or urinary bladder and metastasis to bones and nymph nodes. With aging in men, the prostate gland enlarges. This condition is known as benign Prostatic
hyperplasia, or B P H causes urinary symptoms of obstruction, which may be similar to those produced by prostate cancer. Early stages of the disease are asymptomatic. The symptoms that arise are due
to the growing tumor within the gland.
RY symptoms include frequent and painful maturation, especially during the nights. Difficulty in commencing and maintaining steady urine stream, urinary incontinence, and blood stained urine. There
may be retention of urine and the possibility of renal failure. Other symptoms include. Painful ejaculation, blood stain, semen, weight loss, pain in the abdomen, back pelvis, and other bony areas.
Numbness and weakness of the lower limbs.
Increase in size of the prostate. G. Due to the tumor, which causes pressure on the rectum, causing difficulty in defecation, anemia, compression of the spinal cord, spontaneous pathological
fractures, suppression of bone marrow a age is a primary risk factor. The average age of diagnosis is 70 years. The disease is rare below the age of 40. However, the risk increases as age advances.
Certain ethnic groups such as the African American men are at higher risk as compared to Asian American, Hispanic, and Latino.
Prostate cancer is common in North America, Australia, Northwest Europe and the Caribbean Islands, and less frequent in Africa, Asia, central and South America. The disease has a familial pattern and
occurs in clusters within families. Genes implicated. Are the B R C A one and B R C A two known to cause ovarian and breast cancers in women and ET S genes? ETV one, ETV four and E R G increased the
risk Obesity. And smoking may increase the risk. While earlier, studies implicate vasectomy in younger men as a predisposing factor.
More recent studies rule out a link, vitamins and minerals contribute to the risk of prostate cancer. Elevated serum levels of omega six linoleic and reduced intake of vitamin E. Omega three. Fatty
acids and selenium acid are associated with increased risk. Aspirin, ibuprofen, nrx, and statins reduce the risk of the disease.
Infections such as prostatitis and S t I increase the risk hormones such as insulin-like growth factor one in men increases the risk Early screening using digital rectal examination. And serum PSA
enables early detection. Risk assessment requires routine checkups and testing after the age of 50 in predisposed ethnic groups.
Screening is recommended from the age of 40. A detailed family history indicates the necessity and frequency for testing. General examination accompanied by digital rectal examination, D R E is a
useful evaluation tool Since about 85% of prostate cancers arise in the posterior of the organ, D R E permits evaluation of irregular, lumpy, asymmetric, and hard masses through the rectal.
Laboratory tests such as psa, levels of above four nanograms per milliliter are diagnostic. However, in older men, the PSA levels can marginally increase in the absence of prostate cancer in the age
group of 65 year old. The PSA level of 6.5 nanograms per milliliter is considered worrisome for cancer.
The PSA test is not a specific test, and therefore needs to be combined with tests such as ultrasound and prostatic biopsy to assess the size of the gland. Other molecular markers like D N a, ploy
analysis ein human Cali crane, two micro vessels, density, and P 53 and P 21. Pca, three levels in the urine, et cetera, are also utilized to find out about the advancement of the disease. Other
laboratory investigations such as the complete blood count, coagulation tests, and urine analysis are done as routine diagnostic tests. Although tests such as D R E and PSA are important, the biopsy
determines whether cancer is present.
The procedure is short and can be performed on an outpatient basis using a fine needle or core needle, often performed under the guidance of ultrasound. Biopsies of other sites such as the lymph node
may also be warranted.
The Gleason grading or the Gleason score is used to characterize the aggressiveness of the disease based on the morphology or the extent of transformation of normal prostate cells. A Gleason grade of
one to five is given The Gleason score is used to predict the direction of the disease. Non-palpable cancers may be visualized by imaging studies.
Widely used is Transrectal Ultrasonography, T R U S, CT of the pelvis and abdo. R I and M R s in rectal coil, magnetic resonance imaging, renal sonograms, and plain films are among the other imaging
studies that may be done. A radioisotope bone scan is used in diagnosing metastasis to the bone. Pro skin immuno Scintigraphy scan is performed to identify the spread of the disease to the lymph nodes
and is usually combined with CT to avoid false negative results.
B P H mimics symptoms of prostate cancer. PSA levels are known to rise in B p H and prostatitis prostetic, intra epithelial neoplasia. P I n is clumps of cancer cells confined within the gland,
prostate specific antigen. Psa. Is a serum marker that has revolutionized prostate cancer detection and management. Elevated serum PSA levels are an early indicator of cancer and facilitate early
detection and treatment. The ratio of the free to total PSA may be diagnostically helpful in differentiating between prostate cancer. And B p H of recent interest is the pro enzyme P P S A that has
been identified as potentially the earliest serum marker.
Evaluating the stage of the disease is done using the T N M Tumor nodes metastasis system. That has replaced the older Whitmore DeWit system. It is useful in defining prognosis and determining the
type of treatment. The extent and size of the primary tumor is determined by the T stage, the absence or the presence, and spread to nearby lymph nodes by the end stage. A metastasis by the M stage.
The features and the categories of the TN M stages are as follows, T stage. The T stage is categorized from T1 to T4 and is further subcategorized based on the palpability and tissues involved.
In T1 stage, the tumor is not palpable or visible by imaging, but biopsy reveals cancer tissue T1 is further categorized as T1 A, T1 B, and T1 C. Both T1 A and T1 B stage tumors are accidentally
discovered during trans urethral resection for benign prostate enlargement. While T1 C stage is diagnosed due to elevated P S A levels, T2 stage tumor is confined to the prostate g.
And is detected by direct rectal examination Based on the extent of lobes affected. T2, tumor is subdivided into t2. A half of one lobe involved t2 B, more than half of the lobe, but not both The
lobes are affected and T two C. Both the lobes are affected. During the early T3 stage, the tumor extends to the extra capsular region, covering the prostate gland, spreading to the semial vesicles in
late T3 stage.
Based on the spread of cancer cells, T3 stage is further classified as t3 a t3. And t3. C T4 stage is when the tumor spreads to tissues surrounding the prostate gland, which is grouped as T4 a when
the urinary bladder, neck and sphincter, or the rectum are involved. And T4 B, when the tumor spreads to the pelvic floor, the end stage describes the spread of the tumor or metastasis to the regional
lymph nodes. Metastasis may or may not be present in any of the T stage. Taking into account the number of lymph nodes involved and the size of the tumor. End stage is subcategorized from N zero to N
three. The stage is indicated as N zero when metastasis is absent in the lymph nodes in N one.
Metastasis is found in a single node within the pelvis, and the tumor size is less than two centimeters. If the tumor is larger than two centimeters, but less than five centimeters and is found in one
or more lymph nodes, it is staged as N two in the N three. Metastasis has spread to the lymph nodes and the tumor is larger than five centimeters. The M stage describes the spread of the tumor or
metastasis to other tissues and organs of the body. In M zero stage, the cancer is not spread to other organs and tissues. Well, metastasis beyond the pelvis is staged as M one. The M one stage is
further categorized based on the extent of spread metastasis in lymph nodes outside the pelvis Is M one a stage Metastasis to the bone is M one B.
And metastasis to distant parts such as the liver, lung, or brain is m onec overall, prostate cancer staging is done by combining the TN M staging and Gleason grading systems. Gleason Grading analyzes
the resemblance of cancer to normal tissues and groups them into gx G one, G two, G three, and g4. This combination determines the extent of tissue involvement in cancer and its severity.
Hence, the cancer is divided into four stages. Stage one to stage four. Stage one, cancer is found within the prostate without spread to other tissues and has a low Gleason score. Stage two cancer is
more advanced than stage one cancer. But may involve a part of the lobe, the entire lobe, or both the lobes. The tumor is confined to the gland with a Gleason score ranging between two to 10.
In stage three, the tumor spreads beyond the outer layer of the prostate to the surrounding tissue. Sural vesicles may also be involved. The Gleason score ranges from two to 10. If the cancer has
spread to lymph nodes far or close to the prostate gland or to other organs such as the bladder and the rectum, it is classified as stage four. With the Gleason score ranging between two to 10
prostate cancer, the ninth communist cancer in the world is prevalent in developed countries.
The prognosis, however, in these countries is poor, and therefore nomograms are used to predict outcome. Prognosis is strongly associated with Gleason score and tumor volume. Tumors more than 12 cc
are usually inoperable and tumors less than four cc have good prognosis. Other determining factors are pre-operative PSA level and Gleason.
And the cancer percentage in the biopsy predicts extra capsular extension, extra prostatic extension E P E, or the extension of cancer outside the prostate gland is an unfavorable prognostic
indicator. Prostatectomy is a fairly common surgical option for early diagnosed prostate cancer. Prostatectomy may also be recommended in cases of radiation therapy failure, radical retro pubic
prostatectomy, and radical perineal prostatectomy. Where the incision is through the abdomen and the perineum respectively are usually employed. Laparoscopic radical prostatectomy, L R p, with or
without robotic assistance. Has gained popularity as the surgical incisions are smaller and rarely leave. A scar. L R P may also be performed when radiation therapy is unsuccessful and the debris has
to be removed.
Endocrine therapy or hormonal therapy or androgen deprivation therapy, A D t aim at depleting the levels of androgens that are responsible for the stimulation of cancer cells in the prostate gland.
Testosterone, T and Dihydro Testosterone, D H T. The hormones responsible for the growth and metastasis of the cancerous tissue are blocked. Orchiectomy is the removal of the testicles. This is often
used in cases of spinal cord compression, as it is the quickest method to eliminate the male hormones. Antiandrogens such as Flutamide, Finasteride, nilu, bicalutamide, and Cirone acetate block
hormone receptors within the prostate cancer cells, ketoconazole is and amino thm.
Are medications that can be used as an adjuvant therapy. Use Ofo Trophin releasing hormone agonists such as Buin Trip Tolin. Goin and Leuprolide is a successful therapy. Bernardo Trophin releasing
hormone antagonists such. A relics are also employed, radiation therapy, also known as radiotherapy. Employees ionizing radiation targeted towards cancer cells causing apoptosis. Commonly reported
side effects are diarrhea and rectal bleeding. Radiation therapy also increases the risk of bladder and colon cancer brachytherapy minute radioactive iodine 125 and palladium 103 implants are embedded
within the tumor tissue.
These implants are referred to as seeds. The radiation from these seeds causes the death of cancer cells, external beam radiotherapy, E B R T, or intensity modulated radiation therapy, I M R T is
given over several weeks. The beam size can be varied according to size and shape of the. Thus, preventing damage to the surrounding tissue. TomoTherapy is an advancement over I M R T. The use of
brachytherapy, external beam radiotherapy, and hormone therapy as a triple modality is relatively popular. Cryotherapy is a relatively non-invasive procedure. The prostate cells are frozen to death by
the insertion of a minus 190 degrees Celsius organ called metal rods.
Cryotherapy is a relatively new therapy of uncertain relative efficacy and may be associated with impo. And less frequently urine incontinence, chemotherapeutic drugs such as docetaxel in combination
with prednisone, so Liron radioisotope injections such as Strum 89, phosphorus 32, and Samarium 153. Are targeted towards bone metastasis. Chemotherapy is currently employed as palliative care in
advanced hormone refractory cases of prostate cancer.
It focuses on improving quality and extending life by relieving symptoms of the disease. Hypothermia using 300 megahertz microwaves may have added benefits if applied in conjunction with radiation,
and is also known as thermo radiotherapy in high intensity focused ultrasound, H I F U. Ultrasonic waves of high intensity are converged on target cancer cells. H I F U reduces the risk of developing
impotency and urine incontinence.
Recurrence of prostate cancer after treatment is indicated by increased PSA levels. This is usually due to distant metastasis, usually manifesting as pain in the bones. Some patients may have a local
recurrence in the prostate after radiation, or the prostate bed after radical prostatectomy. For these men, treatment for recurrence is dependent on the initial line of treatment.
Recent advances in diagnostic methods are adenovirus transformed. Luciferase genes are allowed to transfected prostate tumor cells. These infected cells are detected using non-invasive techniques.
Molecular methods are used to detect the presence of PCA three in urine, which is finding worldwide diagnostic application, though non-invasive, this test is not superior to the PSA test.
Early prostate cancer antigen. E P C A two in blood is being researched extensively as it indicates the magnitude of disease, recent advances in treatment of prostate cancer, two chemotherapeutic
agents, Miron and Esra Muk. Have been introduced to stall the progression of metastatic androgen independent prostate cancer, A I P C psa. P A H one, demonstrated selective exterminate of PSA
producing cells. And hence is being evaluated vaccine therapy.
Cousel T is the first among the active cellular immunotherapies. To treat patients suffering from prostate cancer, CT stimulates the patient's own immune system to act against the tumor. Another
vaccine under trial. Is prepared by taking a sample of the patient's own tumor and coaxing it to produce granulocyte macrophage colony stimulating factor. GM C S F. This when readministered
intravenously into the patient, kickstarts a potent immune reaction against the.
Both these vaccines are in the final stages of clinical trials. The increasing incidence of prostate cancer around the world has made researchers work towards identifying new drugs, new regimens, and
new treatment options. That will be beneficial for men with prostate cancer.